
- Medical Specialities
-
- Ahmedabad
- Vadodara
- Anand
-
Call Us
For booking appointments and health check up queries
+91 99 09 02 1667
For Medical Emergency
+91 79 6619 0200
For Information and Inquires
+91 79 6619 0201
For International Patient Inquiry
+91 99090 21667

Finding 'Sanjivani', Daily! (Part-4)
Blog Space / Finding 'Sanjivani', Daily! (Part-4)

- The Motherhood Factor
- The “Higher" Connection
- Man proposes, God disposes
- From Pessimism To Optimism
- Finding 'Sanjivani', Daily! (Part-7)
- Finding 'Sanjivani', Daily! (Part-6)
- Finding 'Sanjivani', Daily! (Part-5)
- Finding 'Sanjivani', Daily! (Part-4)
- Finding 'Sanjivani', Daily! (Part-3)
- Interesting case of pneumonia
- Finding 'Sanjivani', Daily! (Part-2)
- On the moment of 100th Pulmonology Teleconsultation
- Finding 'Sanjivani', Daily
- Why so "Breathless"?
- A Blessing in Disguise
- The Art of Taking Consent
- The Oldman's Pursuit
No. This blog is not about any miracle drug or vaccine against SARS Co-V2 virus responsible for the current deadly pandemic of COVID19. This is regarding the class of medications already invented & used by millions of people across the globe daily - by force or by choice. They are inhaler medications or as commonly called "Pump".
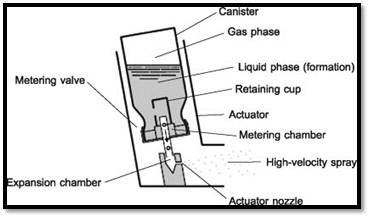
Pressurized Metered-Dose Inhalers (pMDI) are available since 1950s, which revolutionized the aerosol therapy by allowing complete outpatient, portable administration of medication to provide almost instantaneous symptomatic relief. As described in the schematic diagram (see figure below), pMDI consists of canister & actuator. The canisters are typically made from metals such as aluminum or stainless steel & it contains the drug molecule in combination with a mixture of pressurized propellants, preservatives, flavoring agents and surfactants with ability to administer 200 or 120 doses as specified by manufacturer. The heart of pMDI is "metering valve", which ensures a finite and accurate amount (between 25 to 100 micro liters) of formulation per actuation is released at a certain velocity through actuator nozzle of specific 'Orifice Diameter (OD)' when canister is pressed, leading to generation of spray plume to be inhaled in a fraction of a second.
The correct steps are:
- Sit in upright position
- Tilt neck slightly upwards to lift face up
- Shake the device 10 - 12 times
- Remove the cap
- Exhale out completely
- Snugly fit the lips around mouth piece
- Press the canister with thumb/fingers
- Inhale slowly & deeply
- Remove the mouth piece & breath hold for 10-12 seconds or as long as possible
- Repeat maneuver as advised for further dose
- Check the device for remaining dose/dose counter & cap the mouth piece
- Rinse the mouth & throat with water
The seemingly simple steps mentioned above can become cumbersome over long time & lead to faulty inhaler technique. The errors are committed at each step like not shaking the device before use, forget to open the cap before inhaling, but few important steps in my view requires elaboration.
First, the step of pressing the canister requires sufficient force generated with hands, which cannot be exercised by elderly, kids, people with joint problems (like Rheumatoid arthritis etc.) & muscle weakness (like stroke etc.). pMDI is not the device of choice in such population. Second & most important is ability to breathe almost instantly after pressing, also called "Hand - mouth coordination". Poor technique leads to significant mouth-oral (MO) deposition of drug and lesser lung dose leading to suboptimal benefit in symptom control. Adding to that, development of throat irritation, hoarseness of voice, oral thrush are the side effects associated with MO deposition of inhaled corticosteroids, which further discourages regular use of device leading to poor adherence.
In my opinion, pMDI always takes the "examination" of the patient, each time it is used and hence the chances of errors increases in the long term, ultimately requiring modifications and "add-on". Hence, it is mandatory to check inhaler technique in every visit with the Pulmonologist.
As pMDI comes prefilled, it is difficult for the user to estimate how many doses are left. There were many techniques to find out that, such as weight of the canister, floating pattern of the canister, generation of spray plume and ability to taste when inhaled, however those were not accurate, leading to incorporation of "Dose-Counter" in pMDI (see figure below), which basically counts the number of actuations, rather than dose in the canister. They are colour coded and express doses in the countdown manner (120 to 0), some are even digital. A dose-counter incorporated pMDI is always preferred. In resource limited setting, where it is not available, during prescribing pMDI, an estimate of lasting it must be given to the patient.

For example, 1
puff twice daily schedule will need replacement at day 60 in 120 dose device and so on.
With the time, innovations lead to "Breath Actuated MDI (BA-MDI)” (see figure below), which addresses both major limitations of a conventional pMDI: pressing the canister & hand-mouth coordination while keeping the advantages preserved. One just needs to lift up the notch on canister & inhale from the mouth piece while observing all other steps. However, only few molecules are available in BA-MDI limiting its wide spread use.

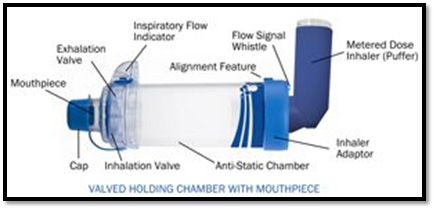
An 'add-on' worth mentioning is Valved Holding Chamber or VHC. They vary in size (from 75ml to 750ml), shapes as well as make (plastic, metal), but they are very effective in reliving patient's 'performance anxiety'. The basic idea is that, after properly shaking & removing of cap, pMDI is attached to VHC in which the spray plume is released and patient can take appropriate time to breathe in. This leads to significantly less MO deposition - particularly a boon for patients requiring inhaled corticosteroid - and ensures proper dosing. The drawback is that, they limit the portability, however if the aim of treatment is to reduce rescue medication, pMDI + VHC remains better alternative for regular maintenance dosing. The other drawback of sticking of drug molecule to plastic surface of a VHC can be easily overcome by appropriate handling & cleaning.
Ultimately, the choice of pMDI, BA-MDI or pMDI + VHC depends on agreement between patient & caregiver after thorough considerations of underlying disease status, inhalation effort as well as cost in long run.
To be continued....
Symbolism : A Pulmonologist passes through lot of thought processes to choose an inhaler just like Hanumanji's struggle to fetch the herb. An optimized inhaler therapy reduces the symptom (particularly of breathlessness) & risk of the disease - just as sanjivani cured army to conquer the evil.
Sanjivani : a miracle herb described in the ancient scripture of "Ramayana", was obtained by Hanumanji after unprecedented struggle. Very few people know that the herb was actually "inhaled" leading to restoration of the army lead by Lord Shri Ram to conquer the evil.
Part-4 of this blog series provides information on how pMDI works along with correct steps to take it as well as discusses Breath Actuated MDI & VHCs.
Dr. Jaykumar Mehta
MBBS (Gold Medalist)
MD, DNB, MNAMS, PD Fellow (Pulmonology)
Consultant Interventional Pulmonologist (Zydus Hospital, Ahmedabad)